点击蓝字关注我们
本文作者:
中国人民解放军南部战区总医院 霍枫教授
前言
肝移植是治疗终末期肝病最有效的方法。然而,供肝严重短缺极大地制约了肝移植的临床应用。为了解决供肝短缺问题也为了进一步扩大供肝池,临床研究使用扩大标准(Extended criteria donation,ECD)供肝。虽然ECD供肝可以部分地缓解供肝短缺的矛盾,但也带来了移植受者安全问题。本文将探讨ECD供肝定义、最新研究进展和未来发展方向。
ECD供肝的定义
ECD供肝指不符合理想供肝选择标准,但依然可以用于移植的肝脏。标准供肝或理想供肝没有确切定义,过去认为应具备以下条件:供体年龄小于40岁,死亡原因为颅脑创伤,脑死亡捐献,器官获取前供体血流动力学稳定,没有脂肪肝或其他潜在慢性肝脏病变,不合并传染性疾病等[1,2]。
相对于上述条件,ECD供肝多认为具备以下特点[3]:高龄供肝(≥65岁),大泡性脂肪肝(≥30%),心死亡(Donation after cardiac death, DCD)供肝,供体ICU停留时间超过7天,合并高钠血症(≥165mmol/L),血清总胆红素超过正常值上限3倍,天冬氨酸转氨酶/丙氨酸转氨酶明显升高,谷氨酰转肽酶≥200单位,供肝冷保存时间过长(≥12h),供体死亡原因为脑血管意外且合并糖尿病和高血压病,供肝获取前供体使用了大剂量或两种以上血管活性药,此外,还包括合并肝炎病毒感染的供肝和劈离式供肝等。
ECD供肝临床应用研究
科学地使用ECD供肝,对进一步扩大供肝池有着重要意义。早期研究认为,高龄供肝肝移植预后具有不确定性,甚至美国医保服务中心(CMS)不建议使用超过70岁的供肝[4]。因此2002年以来,美国此类供肝肝移植占比仅0.15%[4]。然而,新近研究认为,高龄供肝并非是影响肝移植预后的关键因素,而受者年龄(>60岁),既往肝脏手术或移植史和供肝冷保存时间>8h等可能是影响预后的独立危险因素[5]。研究表明控制好高龄供肝冷保存时间,选择恰当的移植受者,优化供受体匹配策略,可以显著改善高龄甚至超过80岁高龄的供肝移植预后[6]。
DCD供肝可能增加移植风险。然而符合以下条件的可控型DCD供肝可以安全地用于临床:供体年龄<40岁,ICU时间<5天,功能性热缺血时间<15min,冷保存时间<8h,没有脂肪变性。新近的研究又提出了ECD-DCD供肝概念[7],即供体年龄>50岁,BMI>35kg/m2,功能性热缺血时间>30min,大泡性脂肪变性>30%,符合其中1项即为ECD-DCD。研究认为科学选择受者,优化围手术期处理方案,可以提高ECD-DCD供肝利用率(52%),改善移植物预后(1年93%),降低缺血性胆病并发症(5%)[7]。
扩大供肝池未来发展方向
近年来,随着对ECD供肝研究的不断深入,尤其是常温下供体局部灌注(NRP)和体外供肝机械灌注(MP)的广泛应用,ECD供肝在临床上的应用也日趋增多。
NRP显著改善了ECD-DCD供肝质量,同时,增加了供体器官获取前功能评估的可能性,极大地提高ECD-DCD供肝利用率。NRP尤其对不可控心死亡供体(uDCD)器官保护有着非常重要的意义[8]。
MP可分为常温和低温机械灌注。常温机械灌注(NMP)可以显著延长供肝保存时限,降低供肝弃用率,减轻供肝的损伤,并且可以科学判断供肝的可用性[9,10]。NMP评价供肝可用性标准包括:胆汁pH>7.5,胆汁葡萄糖浓度≤3mmol/L或低于灌注液葡萄糖水平至少10mmol/L, 维持灌注液pH>7.2,碳酸氢盐补充不超过30mmol, 葡萄糖持续减少超过2h或葡萄糖10mmol/L以下,乳酸峰值下降≥4.4mmol/L/kg/h,灌注2h丙氨酸氨基转移酶<6000U/L。或灌注液乳酸水平低于2.5mmol/L,胆汁产生满意,灌注液pH>7.30,肝动脉流量>150ml/min, 门静脉流量>500ml/min[11,12]。
低温灌注又可分为含氧低温机械灌注(HOPE)和不含氧低温机械灌注(HMP)。HOPE可以显著减轻DCD供肝移植后非吻合口狭窄、术后缺血再灌注综合征、早期移植物功能不全等并发症发生率[13]。新近的荟萃分析表明,HMP与静态冷保存(SCS)比较,能够显著降低早期移植物功能延长恢复(EAD)和胆道并发症的发生率,显著增加移植物1年生存率[14]。
随着NRP和MP技术不断成熟,欧美国家使用NRP和MP保存后再行肝移植的中心日趋增多。新近研究报告,几乎全美各OPO都使用了NRP和MP技术,2016年1月至2021年6月,美国共有374例ECD-DCD供肝经过机械灌注后用于肝移植,移植术后 1年、2年和3年的移植物存活率分别为90.1%、89.1%和87.0%[15]。2015年至2020年,意大利利用NRP联合MP技术,使得DCD供肝利用率提高到了69.2%,取得了满意疗效[16]。
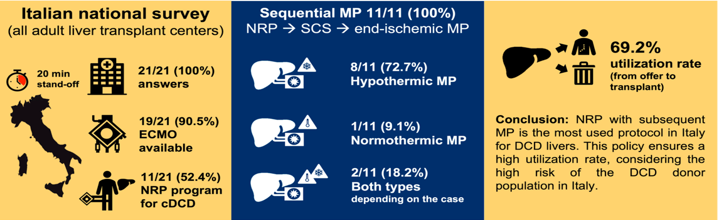
意大利肝移植中心机械灌注应用情况
扫码关注我们
微信号|Tx新方案
健耕医药,专注移植产业